You’re Losing Weight — So Why Is Your Heartburn Getting Worse?
Acid reflux and GERD are supposed to improve with weight loss. And they do — eventually. But in the meantime, a significant number of people on GLP-1 medications find their heartburn getting noticeably worse, not better, particularly in the early months of treatment. New reflux appearing where there was none before. Existing GERD becoming more frequent and more severe. Overnight acid symptoms waking them from sleep.
This isn’t a coincidence and it isn’t bad luck. It’s a predictable consequence of the specific way GLP-1 medications work on your digestive system — and understanding the connection is the first step to managing it effectively.

The Physiology — Why GLP-1 Medications Worsen Reflux
Acid reflux occurs when stomach contents — including gastric acid — move backward from the stomach into the esophagus. The primary defense against this is the lower esophageal sphincter (LES) — a muscular valve at the junction of the esophagus and stomach that opens to let food in and closes to keep stomach contents from moving back up.
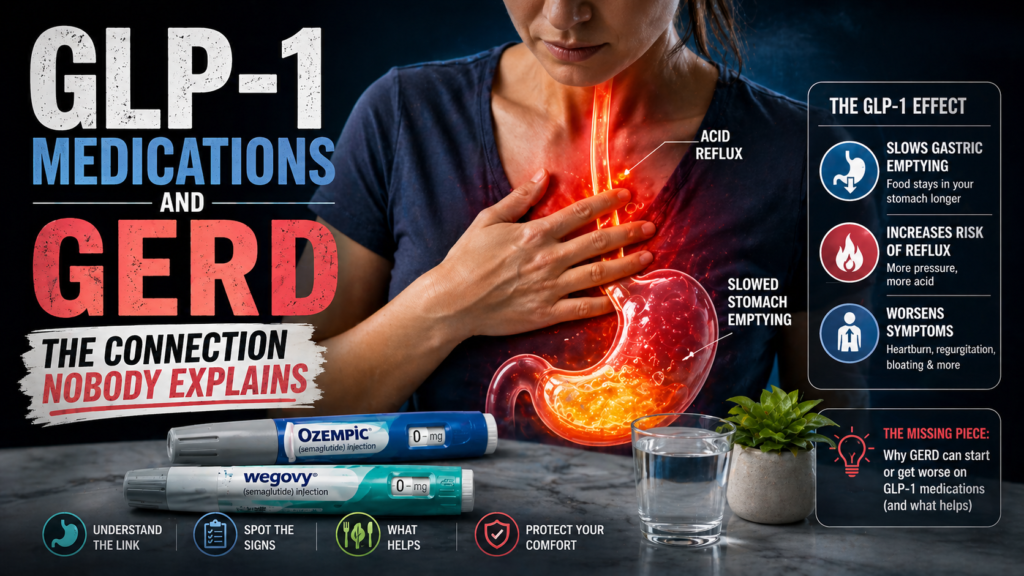
GLP-1 medications create reflux-promoting conditions through several converging mechanisms.
Dramatically slowed gastric emptying. This is the most significant one. When your stomach empties at 30 to 50% of its normal rate, it holds food and acid for significantly longer than usual. More stomach contents held for longer means more opportunity for those contents to reflux upward. A stomach that stays fuller for hours after eating is a stomach that’s generating reflux pressure for hours after eating.
Possible LES pressure reduction. Some research suggests GLP-1 receptor activation may modestly reduce lower esophageal sphincter tone in some individuals — making the valve that keeps acid in the stomach slightly less effective at its job. This effect isn’t consistently demonstrated across all research but is plausible given GLP-1 receptors are present in esophageal tissue.
Increased intra-abdominal pressure from bloating. The bloating that GLP-1 medications cause — from slowed transit and excess gas accumulation — increases pressure in the abdominal cavity. That pressure pushes upward against the stomach, increasing the force that drives stomach contents toward the LES. Bloating and reflux on GLP-1 medications are directly connected — managing one helps manage the other. Why GLP-1 medications cause so much bloating covers the mechanisms that feed into this reflux amplification.
Changed eating patterns. GLP-1 users often eat at irregular times, eat very quickly to minimize nausea, or eat in ways that aren’t optimal for reflux management — lying down shortly after eating, eating late, eating the wrong foods at the wrong times. These behavioral changes compound the physiological ones.
Why It Gets Worse Before It Gets Better
Here’s the important context that makes this situation less alarming: GLP-1-related GERD worsening is typically temporary. As weight loss accumulates — particularly abdominal fat which directly compresses the stomach and LES — reflux should improve significantly. Substantial weight loss is one of the most effective long-term treatments for GERD that exists.
The problem is the gap between starting the medication and achieving enough weight loss to see reflux improvement. During this period — which can be weeks to months depending on how quickly you lose weight and at what dose — the gastric emptying slowdown is producing reflux before the weight loss has reduced the mechanical pressure on your stomach.
Managing the GLP-1 GERD effectively is about bridging that gap — keeping reflux under control while you accumulate the weight loss that will ultimately resolve it.
The Nighttime Problem — Why Overnight Reflux Is Worst on GLP-1s
Overnight reflux on GLP-1 medications deserves specific attention because it’s both extremely common and genuinely damaging if left unmanaged. Gastric acid that spends hours in contact with the esophageal lining overnight — while you’re lying flat and asleep — produces the most significant esophageal irritation and the most serious long-term risks from GERD.
The mechanism is straightforward. On a normally emptying stomach, eating dinner at 7pm means the stomach is largely empty by bedtime — minimal acid, minimal reflux risk overnight. On a GLP-1-slowed stomach, that same dinner may still be sitting in your stomach at 11pm or midnight when you lie down. Lying down removes gravity’s assistance in keeping stomach contents down. The result is hours of acid contact with the esophageal lining while you sleep.
This is why the single most impactful behavioral change for GLP-1 GERD is eating dinner earlier and lighter than you’re used to. Giving your stomach a three to four hour runway before lying down — rather than the one to two hours most people currently allow — makes an enormous difference to overnight reflux on these medications.
The pattern of waking with reflux symptoms or a sour taste connects directly to the morning stomach pain and discomfort that many GLP-1 users experience — the overnight acid exposure sets up a morning that starts with an irritated esophagus and stomach before you’ve eaten a single thing.


Foods That Make GLP-1 GERD Dramatically Worse
The standard GERD trigger food list applies on GLP-1 medications — but the threshold at which these foods cause problems is lower because your stomach is already primed for reflux through slowed emptying. Foods that produced occasional mild reflux before treatment may now produce significant symptoms reliably.
High-fat foods are the biggest issue — they further slow gastric emptying beyond what the medication alone produces, increasing both the duration and pressure of stomach fullness. Fatty meals on GLP-1 medications are the most reliable reflux trigger of any food category. Why greasy food causes so much stomach distress applies directly to the GLP-1 GERD context.
Alcohol relaxes the lower esophageal sphincter directly — reducing the valve’s effectiveness at keeping acid in the stomach. Even modest alcohol intake on GLP-1 medications, which already may reduce LES tone, compounds reflux risk significantly.
Coffee and caffeine stimulate gastric acid secretion and relax the LES. On a stomach that empties slowly with more acid contact time, coffee’s reflux-promoting effects are amplified. Many GLP-1 users find their previously manageable morning coffee habit becomes a significant reflux trigger on the medication.
Citrus and tomatoes are acidic foods that increase the acidity of stomach contents available to reflux. On normally emptying stomachs these are manageable triggers for most people. On GLP-1-slowed stomachs the extended contact time amplifies the impact.
Chocolate, peppermint, and spearmint all relax LES tone through their effects on smooth muscle. These tend to be overlooked because they’re not obviously spicy or acidic — but their LES-relaxing properties make them meaningful reflux contributors.
Large meals of any type — the volume itself is the problem on GLP-1 medications. More food in a slow-emptying stomach means more pressure, more distension, more reflux force. The portion size reduction that helps with nausea helps equally with reflux.
What Actually Manages GLP-1 GERD
Eat Dinner Earlier and Lighter — This Is the Highest-Impact Change
Three to four hours between your last food and lying down. On a GLP-1 medication this is not optional if overnight reflux is a problem — it’s the foundational behavioral change that makes everything else more effective. Shift dinner earlier. Keep it smaller and lower in fat than any other meal. No late snacking.
This single change, implemented consistently, reduces overnight reflux more effectively than any supplement or medication for most GLP-1 users.
Elevate the Head of Your Bed
Sleeping with your head and upper body elevated — ideally 6 to 8 inches — uses gravity to keep stomach contents from moving into the esophagus overnight. A wedge pillow is the easiest practical solution and works consistently for overnight reflux regardless of what’s causing it. Extra pillows under your head alone don’t achieve the same effect — you need the elevation starting from the waist or upper back.
For GLP-1 users with significant overnight reflux this is one of the most important physical interventions available. It doesn’t fix the underlying slowed emptying but it removes gravity as a factor working against you during the hours when you’re most vulnerable.
Sleep on Your Left Side
The anatomy of the stomach — with the esophageal junction on the right side — means that left-side sleeping positions the stomach below the esophageal junction, making reflux mechanically harder. Right-side sleeping does the opposite. If you’re a back or right-side sleeper and GERD is a significant problem on GLP-1 medications, switching to left-side sleeping produces a measurable reduction in overnight reflux episodes for most people.
Manage the Bloating That Feeds Reflux
The intra-abdominal pressure from GLP-1 bloating directly worsens reflux — they’re mechanically connected. Reducing the bloating reduces the upward pressure on the LES. The complete approach to GLP-1 bloating — digestive enzymes with every meal, a quality synbiotic, reduced FODMAP load at dinner — also indirectly reduces reflux by reducing the abdominal pressure that drives it.
Zenwise Digestive Enzymes at the start of every meal reduces the fermentation and gas that creates the abdominal pressure component of GLP-1 GERD. 👉 Check the price on Amazon.
Support Your Gut Microbiome
The gut microbiome influences the esophageal environment through its effects on gastric acid regulation, gut motility, and the inflammatory state of the gut lining. A disrupted microbiome produces a more reflux-prone gut environment. Consistent daily probiotic support with Seed DS-01 maintains the bacterial environment that supports normal digestive function through GLP-1 treatment. 👉 Check the price on Amazon.
Discuss Medication Options With Your Prescriber
For significant GERD on GLP-1 medications that isn’t adequately controlled with behavioral and supplement approaches, discussing acid suppression with your prescriber is reasonable. PPIs (proton pump inhibitors) and H2 blockers reduce gastric acid production — they don’t fix the underlying slowed emptying but they reduce the acidity of what’s refluxing into the esophagus, which reduces the damage and symptoms.
Long-term PPI use has its own considerations — nutrient absorption effects, gut microbiome disruption, and rebound acid hypersecretion when stopping — so this is a conversation to have with your doctor rather than a self-treatment decision. But for people whose GLP-1 GERD is severe enough to be causing significant symptoms or sleep disruption, short-term acid suppression while the weight loss accumulates is a legitimate clinical approach.
Dose reduction or slower titration is also worth discussing if GERD is severe — the reflux effects are dose-dependent, and managing symptoms at a lower dose before stepping up may be preferable to tolerating significant GERD at an aggressive titration schedule.
The Long View — Why Weight Loss Will Help
It’s worth keeping the end goal in view. Abdominal obesity is one of the most significant mechanical drivers of GERD — excess abdominal fat compresses the stomach and LES, generating constant upward pressure that promotes reflux. As GLP-1 treatment produces meaningful abdominal fat loss — which typically happens within the first three to six months of treatment — this mechanical pressure reduces and GERD often improves substantially, sometimes dramatically.
People who had significant GERD before starting GLP-1 treatment frequently find themselves needing less acid suppression medication as their weight loss accumulates. The medication that’s temporarily worsening their reflux through slowed gastric emptying is simultaneously producing the weight loss that will improve it long-term.
Managing the short-term worsening effectively — through the behavioral, dietary, and supplement approaches above — gives you the best chance of staying on the medication long enough to reach the weight loss that addresses reflux at its mechanical root.

Frequently Asked Questions
Why does Ozempic make acid reflux worse?
GLP-1 medications slow gastric emptying significantly — food and acid sit in your stomach for much longer than normal. More stomach contents held for longer means more opportunity for acid to reflux into the esophagus. Bloating from the medication adds intra-abdominal pressure that further promotes reflux. These effects are temporary and should improve as weight loss accumulates.
Does GERD go away on GLP-1 medications?
Eventually — usually yes. Significant abdominal weight loss reduces the mechanical compression on the stomach and LES that drives much of GERD. Most people who achieve substantial weight loss on GLP-1 medications see meaningful GERD improvement. The challenge is managing the worsening that often precedes that improvement during the early months of treatment.
What can I take for acid reflux on Ozempic?
Behavioral interventions first — earlier lighter dinner, elevated head of bed, left-side sleeping, smaller portions. For persistent symptoms discuss PPIs or H2 blockers with your prescriber. Digestive enzymes and probiotic support help manage the bloating that feeds into reflux pressure. Avoid self-treating severe or new GERD without medical evaluation.
Is it normal to get acid reflux on Wegovy?
Yes — it’s reported by a significant minority of GLP-1 users, particularly those with pre-existing reflux tendencies or hiatal hernia. The mechanism is well understood and the side effect is predictable given how significantly these medications slow gastric emptying.
What foods should I avoid for acid reflux on GLP-1 medications?
High-fat foods are the most important to reduce — they further slow gastric emptying beyond what the medication alone produces. Alcohol, coffee, citrus, tomatoes, chocolate, peppermint, and large meal portions are the other significant triggers. All have lower tolerance thresholds on GLP-1 medications than they did before treatment.
Can I take antacids while on Ozempic?
For occasional symptomatic relief yes — antacids are safe alongside semaglutide. For regular daily use, discuss acid suppression therapy with your prescriber rather than relying on OTC antacids indefinitely.

Temporary Worsening, Lasting Improvement — Stay the Course
GLP-1-related GERD is frustrating precisely because it seems counterintuitive — you’re doing something that should help your reflux long-term and it’s making things worse right now. But the mechanism is clear, the management strategies are effective, and the trajectory is toward improvement as weight loss accumulates.
Eat dinner early and light. Sleep elevated on your left side. Manage the bloating that feeds reflux pressure. Avoid the trigger foods that compound the problem. Discuss acid suppression with your prescriber if symptoms are significant. And keep going — the weight loss that’s coming is one of the most effective GERD treatments available.
More from TummyCure:
- Complete GLP-1 Gut Side Effects Guide
- Why Ozempic and Wegovy Make You So Bloated
- Ozempic Nausea Is a Food Timing Problem
- GLP-1 Constipation — How to Beat It
- Should You Take a Probiotic on GLP-1 Medications?
- Living With Acid Reflux
- Home Remedies for Heartburn
- Why Does My Stomach Hurt When I Wake Up?
- The Complete Gut Health Guide
About the Author
Rachel Donnelly is a certified nutritional health coach and gut health writer who spent years struggling with IBS and bloating before making digestive wellness her specialty. She writes for TummyCure with one goal: cut through the noise and tell you what actually works. When she’s not deep in microbiome research, she’s fermenting things in her kitchen and losing arguments with her husband about whether kombucha counts as a dessert.
As an Amazon Associate we earn from qualifying purchases through some links in our articles.